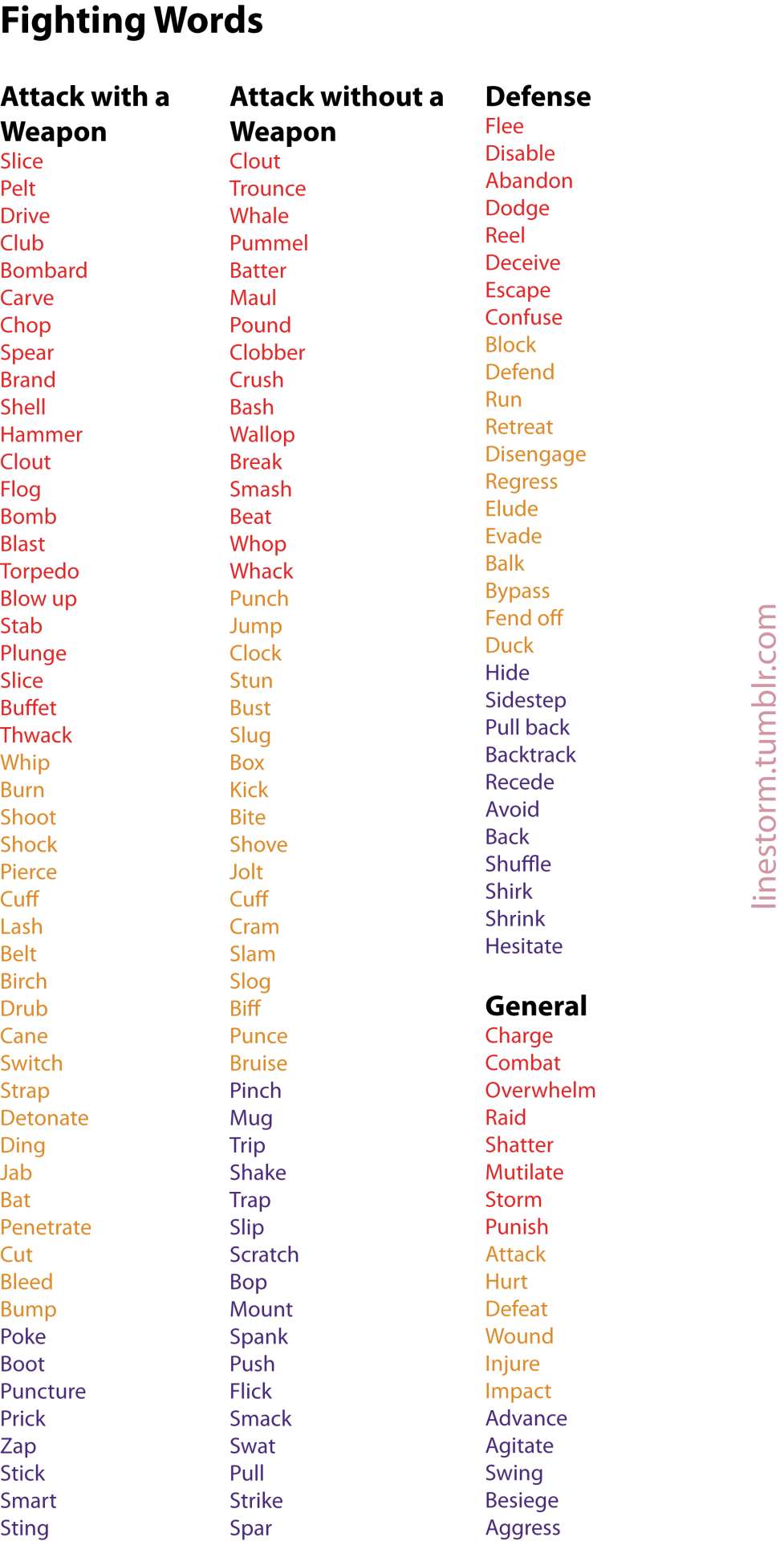
Active verbs to use in a fight scene or an otherwise violent encounter, color-coded by severity (with red as most intense and purple as most mild), and categorized by type of fight.
Hospitals and injury are always such a staple of angst fics, but 9 times out of 10 the author has clearly never been in an emergency situation and the scenes always come off as over-dramatized and completely unbelievable. So here’s a crash course on hospital life and emergencies for people who want authenticity. By someone who spends 85% of her time in a hospital.
Emergency Departments/Ambulances.
Lights and sirens are usually reserved for the actively dying. Unless the person is receiving CPR, having a prolonged seizure or has an obstructed airway, the ambulance is not going to have lights and sirens blaring. I have, however, seen an ambulance throw their lights on just so they can get back to the station faster once. Fuckers made me late for work.
Defibrillators don’t do that. You know, that. People don’t go flying off the bed when they get shocked. But we do scream “CLEAR!!” before we shock the patient. Makes it fun.
A broken limb, surprisingly, is not a high priority for emergency personnel. Not unless said break is open and displaced enough that blood isn’t reaching a limb. And usually when it’s that bad, the person will have other injuries to go with it.
Visitors are not generally allowed to visit a patient who is unstable. Not even family. It’s far more likely that the family will be stuck outside settling in for a good long wait until they get the bad news or the marginally better news. Unless it’s a child. But if you’re writing dying children in your fics for the angst factor, I question you sir.
Unstable means ‘not quite actively dying, but getting there’. A broken limb, again, is not unstable. Someone who came off their motorbike at 40mph and threw themselves across the bitumen is.
CPR is rarely successful if someone needs it outside of hospital. And it is hard fucking work. Unless someone nearby is certified in advanced life support, someone who needs CPR is probably halfway down the golden tunnel moving towards the light.
Emergency personnel ask questions. A lot of questions. So many fucking questions. They don’t just take their next victim and rush off behind the big white doors into the unknown with just a vague ‘WHAT HAPPENED? SHE HIT HER HEAD?? DON’T WORRY SIR!!!’ They’re going to get the sir and ask him so many questions about what happened that he’s going to go cross eyed. And then he’s going to have to repeat it to the doctor. And then the ICU consultant. And the police probably.
In a trauma situation (aka multiple injuries (aka car accident, motorbike accident, falling off a cliff, falling off a horse, having a piano land on their head idfk you get the idea)) there are a lot of people involved. A lot. I can’t be fucked to go through them all, but there’s at least four doctors, the paramedics, five or six nurses, radiographers, surgeons, ICU consultants, students, and any other specialities that might be needed (midwives, neonatal transport, critical retrieval teams etc etc etc). There ain’t gonna be room to breathe almost when it comes to keeping someone alive.
Emergency departments are a life of their own so you should probably do a bit of research into what might happen to your character if they present there with some kind of illness or injury before you go ahead and scribble it down.
Wards
Nurses run them. No seriously. The patient will see the doctor for five minutes in their day. The nurse will do the rest. Unless the patient codes.
There is never a defibrillator just sitting nearby if a patient codes.
And we don’t defibrillate every single code.
If the code does need a defibrillator, they need CPR.
And ICU.
They shouldn’t be on a ward.
There are other people who work there too. Physiotherapists will always see patients who need rehab after breaking a limb. Usually legs, because they need to be shown how to use crutches properly.
Wards are separated depending on what the patient’s needs are. Hospitals aren’t separated into ICU, ER and Ward. It’s usually orthopaedic, cardiac, neuro, paediatric, maternity, neonatal ICU, gen surg, short stay surg, geriatric, palliative…figure out where your patient is gonna be. The care they get is different depending on where they are.
ICU.
A patient is only in ICU if they’re at risk of active dying. I swear to god if I see one more broken limb going into ICU in a fic to rank up the angst factor I’m gonna shit. It doesn’t happen. Stop being lazy.
Tubed patients can be awake. True story. They can communicate too. Usually by writing, since having a dirty great tube down the windpipe tends to impede ones ability to talk.
The nursing care is 1:1 on an intubated patient. Awake or not, the nurse is not gonna leave that room. No, not even to give your stricken lover a chance to say goodbye in private. There is no privacy. Honestly, that nurse has probably seen it all before anyway.
ICU isn’t just reserved for intubated patients either. Major surgeries sometimes go here post-op to get intensive care before they’re stepped down. And by major I mean like, grandpa joe is getting his bladder removed because it’s full of cancer.
Palliative patients and patients who are terminalwill not go to ICU. Not unless they became terminally ill after hitting ICU. Usually those ones are unexpected deaths. Someone suffering from a long, slow, gradually life draining illness will probably go to a general ward for end of life care. They don’t need the kind of intensive care an ICU provides because…well..they’re not going to get it??
Operations.
No one gets rushed to theatre for a broken limb. Please stop. They can wait for several days before they get surgery on it.
Honestly? No one gets ‘rushed’ to theatre at all. Not unless they are, again, actively dying, and surgery is needed to stop them from actively dying.
Except emergency caesarians. Them babies will always get priority over old mate with the broken hip. A kid stuck in a birth canal and at risk of death by pelvis is a tad more urgent than a gall stone. And the midwives will run. I’ve never seen anyone run as fast as a midwife with a labouring woman on the bed heading to theatres for an emergency caesar.
Surgery doesn’t take as long as you think it does. Repairing a broken limb? Two hours, maybe three tops. Including time spent in recovery. Burst appendix? Half an hour on the table max, maybe an hour in recovery. Caesarian? Forty minutes or so. Major surgeries (organs like kidneys, liver and heart transplants, and major bowel surgeries) take longer.
You’re never going to see the theatre nurses. Ever. They’re like their own little community of fabled myth who get to come to work in their sweatpants and only deal with unconscious people. It’s the ward nurse who does the pick up and drop offs.
Anyway there’s probably way, way more that I’m forgetting to add but this is getting too long to keep writing shit. The moral of the story is do some research so you don’t look like an idiot when you’re writing your characters getting injured or having to be in hospital. It’s not Greys Anatomy in the real world and the angst isn’t going to be any more intense just because you’re writing shit like it is.
Peace up.
Ya hear that, Buckley? Loss.jpeg ain’t realistic.
of all the additions and replies on this post so far this is by far my fave.
Thumbs up for this from your friendly neighbourhood physician. (Also, I did mostly emergency care for a few years before switching to radiology. I got the adrenaline junking out of my body before settling down.)
One correction from someone who spent almost a decade working in an ambulance across two states: it is required by law to have your lights on if there is a patient in your rig. Now, this might be a state-by-state law IDK, but in both states I worked in, it was the case. You reserve sirens for Serious Shit because, guess what, they stress out the patient, so unless your patient is crashing in the back of your rig, you don’t run a continuous siren. You are, however, once again required by law to turn on the siren briefly while approaching and driving through stop signs or red lights. (You will also use your siren briefly to get idiots in front of you to move over when you’re stuck in traffic and have a patient whose condition can escalate.)
Also, unrelated to the lights and sirens issue, lemme add a detail about us asking a lot of questions. If you want verisimilitude in your story, remember SAMPLE:
Signs and symptoms
Allergies
Medications
Past illness/injury/disease
Last food, drink, and medication taken
Events leading up to the injury or illness
These are the questions EMTs are trained to ask every patient, though they rarely end up coming out in that order. Also, you can totally add a W to that, which is inevitably “Why did you wait so long to call us?” *sighs forever*
And for some more basic on-scene emergency care, remember CABC: C-spine, Airway, Breathing, Circulation. This time, actually in that order (except for cardiac arrest, in which case remember CAB: Compressions, Airway, Breathing).
The long and short of CABC is: if the patient fell or was in a car accident or had any other potentially traumatic injury, start with stabilizing the C-spine (typically via cervical collar and head blocks and backboard), because if there is a fracture in the neck and you don’t manage it and end up severing the spinal cord that high up, your patient’s probably going to die, and if not, will probably be paralyzed from the neck down.
Once C-spine is stable, make sure the patient’s airway is clear (this includes both foreign obstruction and the patient’s own tongue). Yes sometimes this actually involves sticking your finger in their throat to clear shit out, and yes it’s gross. It also means positioning an unconscious patient’s head in a certain way (assuming there is no chance of C-spine damage) to keep the airway open. EMTs also carry little plastic hook things called oropharyngeal airways in a bunch of sizes that keep the patient’s tongue from blocking their airway. And of course if needs be you can intubate, although this is not a skill EMTs have (paramedics do, though, and in some states there’s a certification called EMT-I [the I for intermediate] that also teaches that skill). If someone’s just come across an unconscious person and doesn’t have an airway to use, and you’re sure their C-spine is fine, you can roll them onto their left side and gently curl them; that’ll help keep the airway clear and also helps the heart pump blood a little more efficiently than if you’d rolled them onto their right side.
Anyway, once the airway’s secure, you move on to making sure the patient is actually breathing. If they’re not, you do it for them with an ambu bag. If they are but are struggling, or aren’t struggling but may for any reason potentially go into shock or have compromised circulation (broken leg, high fever, etc.), you give them supplemental oxygen, typically through a nonrebreather mask, though the flow rate depends on their symptoms.
Okay so once we’ve secured the patient’s C-spine, airway, and breathing, only then do we worry about circulation (unless the patient’s in cardiac arrest, remember, in which case we secure circulation first). Which in the case of trauma is generally first aid for serious open wounds and preventing or treating shock, and in the case of medical issues may be getting an ECG reading or administering medication or, if the patient does go into cardiac arrest, chest compressions and defibrillation.
Okay, that’s the end of the CABCs, but you’ll note that in the last para I said treating serious open wounds. Because a minor open wound is going to wait until after the next step after the CABCs, which is a full-body assessment wherein we meticulously assess a trauma patient using palpation from, basically, head to toe, looking for broken bones, soft tissue damage, internal bleeding, etc. Some of those things can be pretty serious, so before we treat a shallow cut, we check for, like, broken ribs that might puncture a lung.
So obviously not all of these things happen all the time. A patient presenting with an asthma attack needs neither a full-body assessment nor C-spine and circulation management. So we just jump straight to airway and breathing and forego the rest. (And then ask anyone with them our SAMPLE questions if the patient is too distressed to speak, because we still need those answers, but also if the patient is too distressed to speak you can bet we’re asking their companion in the back of a moving ambulance.)
Sometimes you spend a Long Fucking Time at a scene, either because the patient is resisting transport (this happens a lot, especially with the uninsured; we stick around and do everything we can to help them while simultaneously trying to encourage them to go to the ER anyway), or because the patient’s trapped in a smashed car and we’ve got to cut the door off and peel the roof back and get a cervical collar and a backboard on the patient while they’re still in the damn driver’s seat and lemme tell you that is a goddamn game of Jenga and can take half an hour, or because the patient isn’t critical but you want to minimize discomfort and damage so you take the time to meticulously package them while also getting all your questions answered on scene to make sure you haven’t missed anything, or because … well, you get the point. Sometimes shit just takes forever.
Other times, we do what’s called a scoop-and-go, typically with patients in critical conditions that can’t really be managed without surgery or medications we don’t carry. Like, patient bleeding out while giving birth? Not a whole lot we can do about that, so we get them in the rig as fast as fucking possible and race to the hospital while trying to get the most critical questions answered. These kinds of situations are very rare, though; it’s much more common to be on scene for 15 or 30 minutes than 5 minutes.
OH AND, another thing. Listen. EMTs do not approach a scene that is not secured. If there’s an active shooter, or a hostage situation, or a raging fire, or a potential for something to explode (or for something that’s already exploded to collapse), or a flash flood, or a hazardous materials spill, or whatever else, we do not go in until the unstable situation has been resolved. It sucks waiting 100 yards away while a critical patient is maybe dying and you can’t get to them yet, but listen, the first thing they teach you is don’t make new patients. IOW, don’t become a victim yourself; you can’t help anyone if you get wounded in the crisis too, and in fact then you’ve just become an additional burden on the personnel remaining.
Okay, so, any questions?
ALL OF THIS. With one exception to what @rachelhaimowitz added, which is:
I’ve never heard of the lights-must-be-on rule. It’s gotta be one or a few specific states. Generally speaking, lights and sirens increase accident rates, and most states are actively trying to REDUCE their use, not increase them, but I don’t know where she lives, so that’s accurate in her part of the country (I’m assuming the US). But it’s inaccurate in most of the country.
xoxo, Aunt Scripty
the number one thing i think writers consistently get wrong is this:
it’s hard work being a patient.
you don’t blissfully black out at the scene and wake up in a clean white room with everything fixed. depending on the specifics, you can be awake and functioning through absolutely ridiculous levels of pain. ask me how i know. except don’t. i don’t want to talk about it. you can be a complete disaster area, and you’ll still have to answer questions. unless you’re actively dying this minute, someone will interrupt your sobbing and vomiting to ask for your insurance card. you’ll have to describe your symptoms even if they seem obvious. you’ll have to get your blood pressure and temperature taken, possibly multiple times, even if you’re curled in a whimpering ball. these are procedures they don’t skip.
there won’t be soothing words and back pats. your dignity is not the medical workers’ concern. they are going to be as efficient and proper as possible about helping you. they may or may not be kind about it. they’re not going to wait while you have dramatics over the situation, certainly; whoever you brought in with you is going to get kicked out if they’re keeping you from cooperating with care.
there’s a lot of waiting even when things are moving along briskly – you’ll get left in a room while people do things where you can’t see. you’ll feel lonely and neglected. it can be tremendously scary, wondering if maybe they just forgot about you, even though you’re sure they wouldn’t.
throughout it all, you will be ugly. you’ll be dirty and smelly. your hair will be messed up and sweaty. if you were wearing makeup when you got sick/injured, it’s now smeared hilariously across your face. whatever blood/vomit/urine/whatever you get on yourself, you’ll be wearing it until you’re well enough to shower. the emergency room isn’t a spa, nobody’s coming with a loofah. you get to stay gross.
and you don’t get to just lie there. if you physically can move, you’ll be expected to. you can get help, and ride in a wheelchair if walking’s hard, but you’ll undress yourself and put on your own smock, you’ll get onto and off of the cot yourself, you’ll turn over so they can see your other side, all that good stuff – you’re present and participating, no matter how distressed.
you won’t even get a painkiller until after quite a lot of investigation. you definitely won’t get knockout drugs unless you’re going directly into surgery.
oh, and being intubated kinda rips up your throat, so you won’t be very chatty after surgery either.
the kind of hospital scene where our hero goes directly from the gunshot to waking up wan but clean, and everyone gathers around to discuss the next plot item, drives me extra batshit after my recent hospital adventures. not that i guess you particularly want to watch a movie where they devote much screentime to being catheterized, but let’s at least dispense with the ‘blurry semi-conscious face on the gurney and then blackness’ bit, and maybe have some characters babbling like drunks, or making the war face to keep from hollering, or in some way reacting individually to being afraid and in pain.
one thing that’s less unpleasant than fiction makes it – for your usual sort of ‘i got fucked up’ emergency room visit, if you’re not getting rushed into surgery, they don’t forbid people other than blood family or a legal spouse from coming with you. if your best friend or coworker or some random samaritan brings you in, you can have them sit with you while you get stitched up. basically, as long as they’re being helpful and not disruptive, you probably won’t get any objections. you can only have one person, though, apparently; my last visit i had both my spouse and my home care person, and when it got down to brass tacks one of them had to go back to the waiting room. i think just because the exam rooms aren’t very big.
Leveraged an inventory of established fictional character and setting elements to generate a disruptive custom-curated narrative entertainment asset.
I worked in HR, handling applications and interviews, and if someone turned in that string of techno babble nonsense, I would have rejected them out of hand.
A resume doesn’t need to sound fancy or overly technical, it needs to tell us why we should hire you.
“Independent novelist/writer” is more than sufficient here. If you want to express the skills that fan fiction taught you, something like, “creative writing, editing, and publication,” will get you a lot further than… Whatever that just was.
A resume should be tailored to the position, if you can afford the time and energy for that. But if not, then just think about what writing got fandom taught you. How to respond to criticism, how to present a professional pubic face, how to correct punished mistakes, creative thinking, project planning, persuasion via emotional leverage, html formatting, office suite fluency.
There are a lot of actual, marketable skills that go into fan fiction.
How to put “I was in a zine” on your resume
Writer:
Published short fiction stories for anthology collection
Able to write short fiction within a designated word count for layout purposes (900-1500 words, 1500-2000, 3000-5000)
Wrote short articles for independent publication
Assisted with editing short stories for publication
Able to reduce or expand written content based on layout needs
Able to check for basic spelling, grammar and syntax
Familiar with Microsoft Office and Google docs
Artist:
Produced full-colour digital illustration for independent magazine
Able to produce digital illustrations optimized for both online and print display
Produced full-colour 2-page spread for art anthology
Published 4-page short comic in anthology collection for charity
Able to transfer traditional art to digital illustration
Illustrated the cover (always brag if you’re on the cover) of an independent art publication
Familiar with professional illustration tools such as Adobe Photoshop, Illustrator, Clip Studio Paint and stylus tablet
Merch artist / graphic designer:
Designed 2″ clear decorative double-sided keychain charm as bonus sale item
Designed 5″ x 6″ sheet of graphic stickers included in art anthology
Able to design bold graphics that are measured for laser cutting production
Designed layouts for 65-page art and writing magazine, focusing on (art placement, text layout, etc)
Able to keep layout design simple and in accordance with the project director’s chosen theme
Created promotional art, icons and banners tailored for social media sites like Twitter, Tumblr, Facebook, etc
Familiar with professional layout and design software such as Adobe Illustrator and InDesign
Running a zine
Produced an independent art and writing collection for sale / for charity
Managed (10, 20, 30) independent artists and writers out of over 500 applicants to create a short-run independent magazine
Worked in online sales and social media promotion selling an independent comics anthology
If it’s really spectacular you can brag about specific numbers
Our book raised over $4,000 for charity in under six months of production
We sold over 750 copies in two weeks of online sales
Produced a digital PDF and printed version of anthology, mailing to recipients all over the world
Communicated with printers and manufacturers of plastic accessories and paper goods, assembling professional packages of our merchandise for mailing.
Built a custom digital storefront and navigated professional market and payment systems including Paypal and Tictail / Bigcartel / Wix etc
Created promotional events to boost sales, including raffles and giveaways over social media
Organized participants through mass emails and use of social media posts on tumblr and twitter
Familiar with organizational software such as Microsoft Excel, Google spreadsheets and Trello
Added some more
Also if you have ever beta’d
Freelance copy editing experience. Providing constructive feedback. Ensuring writing meets the highest grammatical standards. Maintained consistency throughout narrative by checking spelling, syntax and brand standards.
This is timely, because I literally just was working on a friend’s resume who does commissions on tumblr, and I wrote it like this:
Freelance Artist • Created custom artwork for a variety of domestic and international clients. • Communicated effectively with customers in order to facilitate and execute their visions according to their individual needs. • Invoiced and processed payments via PayPal processing service. • Met deadlines, sustained a high level of customer satisfaction, and cultivated a database of clients. • Used social media to find and connect with customers.
Never underestimate the work that you’re doing!
Oh, yes, my friends. The earlier you learn to sell yourself with unmitigated bullshit, the better off you’ll be.
But its not bullshit. Really. You *do* all of those things, but since you don’t do them in an “approved” setting (i.e. work) we’ve been conditioned to discount them.
Professionally, I am a senior solutions technician for custom software designed for the bottling industry. In English – I work a help desk for a very small software company with very large clients, and I’ve worked there a really long time.
I am also manage the logistics, accounts receivables and an responsible for creating and maintaining a budget and long-term financial planning for a group of four, as well as meet transportation needs, medical supply orders, and resolve conflicts between those same four people. I am also on call 24/7 for emergency services including, but not limited to, transportation issues, scheduling conflict, limited medical issues and escalation to specialists if needed. In English – I’m a mom with a spouse and two kids. My responsibilities in the house are paying the bills, helping to manage my son’s diabetes, his and my husbands mental illnesses, make sure that everyone has a ride to all of their extra-curricular activities, etc. Since I don’t get paid for that, it doesn’t count, even though all of those skills are directly applicable to the workplace.
the greatest skill a woman can learn for herself is self reliance
to clarify … so many strong women in my life rely on men. that dependence is dangerous. ladies here are some good ref resources I’ve found helpful on my journey towards self reliance